What is the orthopaedic surgeon’s role in preventing escalation of a national crisis?

By Vani J. Sabesan, MD; Danielle Malone, MPH; Kiran Chatha, MD
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Ninety Americans die of an opioid overdose daily, and while the United States represents only 5 percent of the global population, it is responsible for 80 percent of global opioid consumption and use 99 percent of the global hydrocodone supply. Opioid abuse is a systemic and pervasive problem that presents a challenge for all medical specialties and especially orthopaedists, whose patients often require marked pain management postoperatively.
Orthopaedic surgeons are the third-highest prescribers of opioid-based medications. Recognizing our role and responsibilities in balancing pain management with helping patients avoid opioid dependency, a group of forward-thinking Cleveland Clinic Florida physicians is looking at ways to stem the tide.
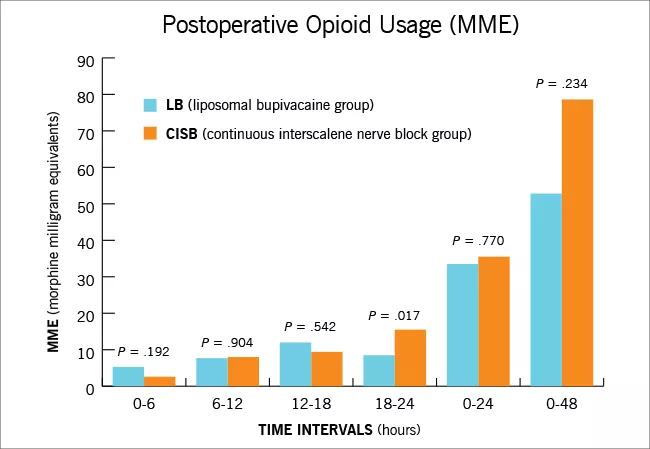
Growth rates of total shoulder arthroplasty (TSA) are comparable to those of total hip and knee procedures in the U.S. As these numbers rise, postoperative pain management and optimization of outcomes are critical. Multimodal pain management is the current standard of care for TSA patients, incorporating anti-inflammatories, opioids, other analgesic medications and regional nerve blocks. One option for non-narcotic extended postoperative pain management is continuous interscalene nerve blocks (CISB). These have many advantages, but associated risks have led to exploration of alternatives, such as long-acting liposomal bupivacaine (LB). This agent has gained popularity for its potential to provide extended postoperative pain relief with fewer side effects.
We performed a prospective, randomized clinical trial to assess the efficacy of LB, and found significant reduction in opioid use at 18-24 hours after surgery (P = 0.017). The LB group had equivalent narcotic usage, pain scores and time to first narcotic rescue compared to the gold standard CISB group, but with fewer complications and cost, demonstrating that LB provides an excellent option for postoperative pain relief for shoulder arthroplasty patients (see chart below).
To further delineate the effects of narcotic usage, we evaluated previous narcotic usage in a lower socioeconomic population undergoing rotator cuff repair. Preoperative opioid use has been correlated to suboptimal outcomes after orthopaedic surgeries. We found that opioid-dependent and opioid-naïve patients had significant improvements on all patient-reported and functional outcomes. However, the preoperative opioid-naïve patients demonstrated significantly better postoperative patient-reported outcome scores. Within the opioid cohort, Medicaid patients reported significantly lower subjective shoulder scores compared with non- Medicaid patients. Regardless of payer status, preoperative opioid use negatively impacted functional outcomes for all patients undergoing rotator cuff repairs.
To better understand who develops postoperative opioid dependence, we developed a narcotic outcome database for TSA patients. We are examining over 2,000 patients who underwent shoulder surgery at Cleveland Clinic to understand how risk factors and diagnoses relate to postoperative dependence. Some clear trends have already emerged.
Orthopaedic patients are oftentimes already narcotic-dependent upon initial presentation, and we may be overprescribing narcotics pre- and postoperatively. Our results also indicate that a majority of patients do not take all of the pills prescribed and report taking their narcotic medication only immediately postoperatively. We found a 3.5 times greater risk for postoperative dependence when TSA patients took narcotics for more than one month preoperatively. In the trauma population, we found that the management of upper extremity fractures with narcotics for extended periods of time prior to surgery may cause increased postoperative dependence and prolonged, higher doses of narcotics.
Inspired to decrease narcotic dependence in the orthopaedic population, we are seeking funding to launch a narcotic-free campaign that will begin with the creation of educational materials and development of a validated, narcotic-free postoperative pain management protocol that surgeons can use confidently.
While creating a narcotic-free campaign in this population may seem a daunting task, we are confident that our unique protocol will facilitate success. Through educational tools and focus groups, patients will learn the implications of using opioids and that postsurgical pain can be managed effectively without narcotics.
We hypothesize that patients electing to forgo narcotics will have less dependence, equivalent functional outcomes and higher satisfaction levels compared with the narcotic group. If successful, our campaign will be extended to the much larger Cleveland Clinic total joint arthroplasty population.
Reversing the opioid crisis will take time, but orthopaedic surgeons at Cleveland Clinic Florida recognize that with the number of primary arthroplasties projected to jump to 3.5 million by 2030, now is the time to start.
From the Levitetz Department of Orthopaedic Surgery, Cleveland Clinic Florida, where Dr. Sabesan is an orthopaedic surgeon, Ms. Malone is a research coordinator and Dr. Chatha is a clinical research fellow.
Burkhart SS, Ricchetti ET, Levine WN, Galatz LM. Challenges and controversies in treating massive rotator cuff tears. Instr Course Lect. 2016;65:93-108.
Sabesan VJ, Shahriar R, Petersen-Fitts GR, Whaley JD, Bou-Akl T, Sweet M, Milia M. A prospective randomized controlled trial to identify the optimal postoperative pain management in shoulder arthroplasty: liposomal bupivacaine versus continuous interscalene catheter. J Shoulder Elbow Surg. 2017;26(10):1810-1817.

Cleveland Clinic specialists offer annual refresher on upper extremity fundamentals

Latest concepts in the surgical creation of functional, opposable thumbs in early childhood

CT imaging using radiopaque markers can help assess healing after surgery

Finally, a solution after multiple revision surgeries for delayed bone healing, loose hardware and unrelenting infection

Iliac crest structural autograft repairs large, uncontained defect
Two cases show multiple factors to consider

Orthopaedic oncologist discusses the complex case

Data system aims to improve orthopaedic care and drive down healthcare costs